Types of patients with hypothyroidism
Some patients with hypothyroidism can be challenging to treat and require special consideration. Use this section to review the cases of Steve, Jennifer, and Diana to see how to effectively manage their hypothyroidism with Synthroid (levothyroxine sodium).

Steve, 50
Recently diagnosed patient*
- Recently diagnosed with hypothyroidism
- Initiating treatment

Jennifer, 32
Pregnant patient*
- Diagnosed with hypothyroidism 3 years ago
- Started and managed on levothyroxine

Diana, 70
Elderly patient*
- Diagnosed with hypothyroidism 10 years ago
- Gastroesophageal reflux disease (GERD) diagnosed 6 months ago
Past Medical History:
- 4 months ago, 190-lb patient presented with weight gain of 20 pounds in 1 year. Patient complained of fatigue, dry skin, constipation, cold intolerance, TSH 10.2 mIU/L, BP 150/60, total cholesterol 235 mg/dL; patient was diagnosed with hypothyroidism and started on Synthroid 137 mcg
- 8 weeks later, patient’s complaints continued. TSH 4.6 mIU/L; Synthroid dose increased to 150 mcg
Current Complaint:
- Nervousness, agitation, palpitations, and feeling hot for the past few months
Current Medications:
- Synthroid 150 mcg
Notable Physical Exam and Lab Findings:
- Sweating profusely despite air-conditioned exam room
- TSH 0.3 mIU/L
Diagnosis:
- Patient is displaying symptoms of being overreplaced with current dose of Synthroid of 150 mcg; TSH test confirmed
Treatment Plan Considerations:
- Decrease dose of Synthroid
- Recheck TSH levels in 4-6 weeks
*Hypothetical patient profile.
Clinical insights
- Managing hypothyroidism requires frequent monitoring
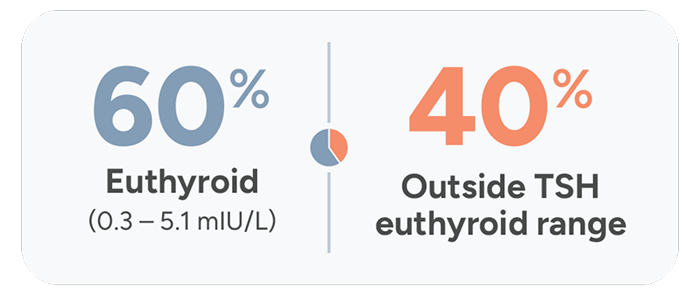
- Study of more than 1500 patients found that 40% of patients being treated for hypothyroidism were not within the normal therapeutic TSH range15
Many patients on thyroid medication struggle to reach optimal TSH levels15,16
The Colorado Thyroid Disease Prevalence Study
The Colorado Study, a cross-sectional study of patients (N=25,862) at a statewide health fair in 1995, found that only 60% of hypothyroidism patients receiving replacement therapy had normal TSH levels.
25 mcg
orange
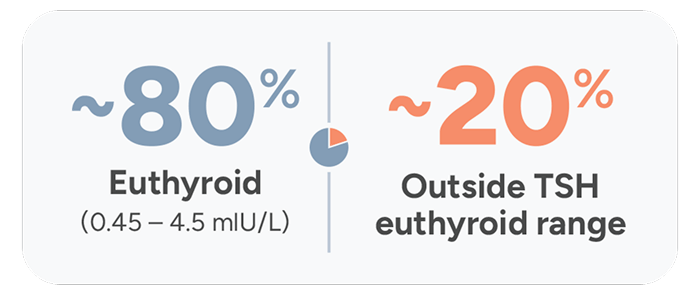
Treatment Adequacy Study
A retrospective Treatment Adequacy study was conducted between 2013-2020 and found that over 20 years later, ~20% of patients taking thyroid medication still do not achieve normal TSH levels.
25 mcg
orange
Overall, 81.1% ([CI: 80.4-81.8]; N=9130) of patients had normal mean TSH levels and 11.7% [CI: 11.1-12.3; N=1312] and 7.3% [CI: 6.8-7.8; N=817] had high and low TSH levels, respectively.
Achieving steady TSH levels and hormonal stability requires precise, individualized dosing, and adequate monitoring is essential in stabilizing TSH levels.2
- Under- or overmedicating can have serious effects2
- With a narrow therapeutic range, even small dose changes in levothyroxine, including Synthroid, can affect TSH levels2
The Carr study: proof that precise dosing matters17
Adapted from a 1988 biochemical study conducted in 21 adult Caucasian patients in the United Kingdom with primary hypothyroidism who were tested on a series of different thyroxine dosages to evaluate effectiveness of measuring TSH levels to monitor thyroid function.
Effect on TSH levels of 25-mcg change in levothyroxine dose17,18

Pregnant Patient*
Jennifer is a 32-year-old woman in her first trimester of pregnancy with hypothyroidism that is managed on Synthroid.
Past Medical History:
- Diagnosed with hypothyroidism 3 years ago
- Started and managed on 50 mcg Synthroid
- Weight fluctuation
- Appendectomy
Current Complaint:
- Fatigue and facial puffiness
Current Medications:
- Synthroid 50 mcg
Notable Physical Exam and Lab Findings:
- Young woman with cold, dry skin and facial puffiness
- TSH 6.2 mIU/L
Diagnosis:
- Patient is displaying symptoms of hypothyroidism due to subtherapeutic dosing of Synthroid; TSH test confirmed
Treatment Plan Considerations:
- Increase dosage of Synthroid
- Recheck TSH levels in 4 weeks
*Hypothetical patient profile.
Clinical insights
TSH levels may increase during pregnancy. TSH should be monitored and Synthroid dosage adjusted during pregnancy.1
- 2017 ATA Guidelines state that19:
- Between 50% and 85% of treated hypothyroid women need to increase their levothyroxine dosing during pregnancy
Elderly patient*
Diana is a 70-year-old woman who has a history of hypothyroidism that has been managed on 112 mcg of Synthroid for the past 5 years.
Past Medical History:
- Hypothyroidism diagnosed 10 years ago
- Gastroesophageal reflux disease (GERD) diagnosed 6 months ago
- Enlarged thyroid
Current Complaint:
- Increasing hair loss, fatigue, chronic constipation for the past few months
Current Medications:
- Synthroid 112 mcg
- Daily fiber supplements
- Proton pump inhibitor (PR)
Notable Physical Exam and Lab Findings:
- Well-nourished elderly woman with thinning hair
- TSH 5.7 mIU/L
Diagnosis:
- Patient is displaying symptoms of hypothyroidism (TSH test confirmed), most likely due to the initiation of a PPI and the concurrent use of daily fiber supplements
Treatment Plan Considerations:
- Counseled patient to take Synthroid on an empty stomach and at least 4 hours before or after other medications
- Recheck TSH levels in 6-8 weeks
*Hypothetical patient profile.
Clinical insights
